
In a historic decision on December 15th, the UK legalized the creations of “three person babies” in an effort to prevent debilitating, even fatal, mitochondrial diseases1.
Earlier this year, the first “three person baby” was born in Mexico to a Jordanian mother who carries the gene for Leigh syndrome, a mitochondrial neurological disorder that causes progressive loss of movement and deterioration of mental functions. The term “three person baby” is misleading because it alludes to one child made in three equal parts, however, most of the genetic information in this technique is from two parents with a tiny amount from a woman donor.
This methodology is called, “Maternal Spindle Transfer” (MST), where there are two eggs: one from the mother-to-be and one from the donor woman. The nucleus of the maternal egg is removed from its cytoplasm, which is diseased by pernicious mitochondria. Her nucleus is then transplanted into an undiseased cytoplasm containing healthy mitochondria.
Cytoplasmic mitochondria code for only about 30 genes, compared to the 30,000 genes coded for in the nucleus. The DNA in the nucleus is known to code for “personality” traits, among many other traits, whereas the cytoplasmic mitochondria are known to code only for energy production2. This fact was used by MST proponents in an effort to assuage concerns for one child with an identity split three ways.
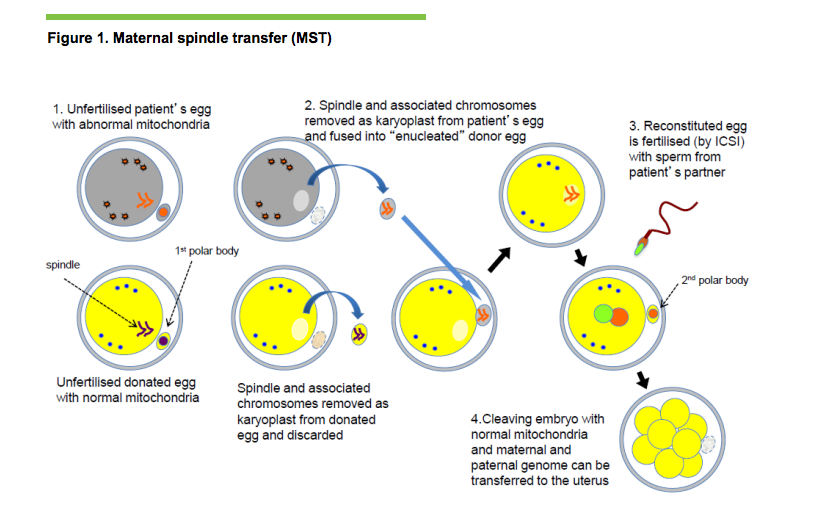
MST has been in trials since the 1990’s and this was its fourth scientific review in half a decade by government run Human Embryology and Fertilization Authority (HEFA). While MST was approved on December 15th as “sufficiently safe” for humans, concerns remain. The largest problem outlined in HEFA’s report is that some of the diseased mitochondria (0.1-1%) is attached to the spindle and carried over into the donor cell. Less than 2% of diseased mitochondria is normal even in somatic cells and are not known to cause problems. However, this mitochondrial may replicate, which would either negate the procedure or the diseased mitochondria could interact with the healthy mitochondria in dangerous and unpredictable ways3. Additionally, there is a theoretical possibility that in transfer chromosomes can fall off the spindle and create a diseased child. Finally, it is a reality that mitochondria are not entirely understood. While scientists believe that personality traits stem exclusively from the nucleus, as always in science, there is still reasonable doubt on the full impact of donor DNA on the child’s development.
That being said, “complete reassurance will never come from experiences conducted in animal models and human material in vitro”2. For this procedure we have learned everything we can from animals. We must now safely practice what we have learned and found to be effective on humans, otherwise this life saving procedure will never be implemented. There will be risk and uncertainty with the use of MST until we understand it fully in humans. This is the case with all research that moves from animals to humans.
A common fear in public discussion is taking embryonic alteration to its logical conclusion- to “designer babies”. This snowball argument claims that if we allow any embryonic alteration, eventually we will be practicing a form of eugenics of choosing our child’s traits4. This would be a dystopian world where the rich choose physical traits of the most valuable humans and impose those values upon the future generation. While understandable, holding firm to this fear prevents a cure to a child’s terrible disease. MST has no ethical problems once it is understood as preventive medicine as a tissue transplant. Nuclear transplants remain illegal. The goal is not to create a super human; the goal is to create a human who has the same chance of survival as you and me.
At this time, MST is going to proceed cautiously and slowly, with only 25 women (and unborn babies) treated a year1. These women will apply, be screened, and given a license from HEFA to proceed with treatment.
MST has been influencing how we perceive identity in the 21st century. The Department of Health ruled that the donor woman, some would say donor mother, and the child have no contact because they have no significant genetic relationship. The Department of Health is doing this to prevent complex or unwanted relationships. Catholic ethicists argue that this form of creating children, “dilutes parenthood,” and are worried about a break in the child/parental identity5. Oddly, the church’s statement appears to glaze over parents and children in atypical situations- such as adopted families. Is the parenthood of those children who need a home diluted as well because of their lack of genetic relation? What about parents of children who need a heart or skin transplant? Regardless, the Catholic Church would reject MST, because as John Paul II stated in the Dignitas Personae, “to create embryos with the intention of destroying them (in this case the donor embryo), even with the intention of helping the sick, is completely incompatible with human dignity, because it makes the existence of a human being at the embryonic stage nothing more than a means to be used and destroyed.”6
Although the Catholic Church is against MST, the Church of England stated that is is not necessarily opposed, but they want more research and discussion on ethical repercussions. This is a surprising shift considering in 2008 the church released a statement that, “the status of the embryo…has the same right to protection that is accorded to early human life, on the basis of the traditional respect for the sanctity of that life.”6
HFEA recommends that women are offered prenatal testing after the procedure if they desire to know the efficacy of MST2. If the procedure fails and the child has a mitochondrial disorder, some women may abort the fetus. If a woman decides to abort her fetus with a mitochondrial disorder, would that be considered early euthanasia? Would an abortion symbolize how an individual and society values mitochondrially diseased or even disabled children? Or is it just compassion? To avoid eugenics, we have a moral imperative as a society to carefully consider the value that we place on humans who are healthy versus those that have diseases. We cannot sprint towards a medical innovation merely because it is useful or the most utilitarian thing to do. We must carefully walk the grey line of asking ourselves what a good quality of life looks like, how to equally value all humans, and to what extent will we go to prevent disease. We must not become socially complacent, as it is so easy to do, and continually return to these difficult questions.
The legalization of “three person babies” in the UK has propelled much classical, textbook bioethical conversation into the public sphere. Society, or at least the UK’s society, is being forced to consider basic questions of identity, how far will we will let technology go to heal people, the ethical reasoning of abortion, and cost benefit analysis of millions of government dollars funneled to embryos.
I think that this technology has incredible potential for saving unborn children from a lifetime of tragic health problems. Through MST, we are finally beginning to take hold of the furthest reaches of preventative medicine. It is an incredible feat, a manifestation of a social pact prevalent throughout the UK that prioritizes a healthy and thriving society. I am unsurprised that the UK, a place with governmental paid maternity and paternity leave, is pioneering MST. It is the continuation of a simple social principle, when we invest in rearing our children, we secure our country’s future.
References:
Gallagher, James. "Babies made from three people approved in UK." BBC News. December 15, 2016. Accessed December 16, 2016. http://www.bbc.com/news/health-38328097.
United Kingdom. Human Fertilisation and Embryology Authority .Scientific Review of Safety and efficacy of methods to avoid mitochondrial disease through assisted contraception: 2016 update.By Andy Greenfield. 2016. Accessed December 16, 2016. http://www.hfea.gov.uk/docs/Fourth_scientific_review_mitochondria_2016.PDF.
Callaway, Ewen. "Three-person embryos may fail to vanquish mutant mitochondria." Nature: International Weekly Journal of Science. May 16, 2016. Accessed December 16, 2016. http://www.nature.com/news/three-person-embryos-may-fail-to-vanquish-mutant-mitochondria-1.19948.
Diamond, Rebecca. "Social and ethical issues in mitochondrial donation."Oxford Journals 115, no. 1 (2015): 173-82. July 27, 2015. Accessed December 16, 2016. doi:10.1093/bmb/ldv037.
Blackman, Daniel. "Embryo Expert: UK Will Have First ‘Three-Parent’ Child in 2017." National Catholic Register. December 13, 2016. Accessed December 16, 2016. http://www.ncregister.com/daily-news/embryo-expert-uk-will-have-first-three-parent-child-in-2017.
"Therapeutic Cloning." RS Revision. 2015. Accessed December 16, 2016. http://www.rsrevision.com/GCSE/christian_perspectives/genetics/therapeutic_cloning/church.htm